“Live as if you were to die tomorrow. Learn as if you were to live forever” said Mahatma Gandhi.
Learning everyday is so essential to life.
In a profession like ours that is responsible for people’s lives and well-being, transferring the right information to the right people at the right time is even more vital.
Secondly, surgical technology and techniques advance rapidly. Unless the early adopters of a good technology diffuse it vigorously to the rest of the fraternity, majority of patients will always be deprived of better care and treatment.
Hence continuous learning is essential for surgeons all through their career span of 30 to 40 years.
I was an early adopter of Laparoscopic or Keyhole Surgery in 1990s with a handful of other Indian surgeons. My conviction that Keyhole Surgery has immense benefit over open surgery motivated me to embrace it, gain experience, develop techniques, and then train other surgeons interested in acquiring those skills.
Why should a private practitioner train others? Aren’t Medical Colleges and Universities supposed to do it?
Medical colleges and teaching hospitals stick to the prescribed syllabus to teach basics. Also they work under resource constraints, which makes it often difficult for them to allocate budgets for adopting latest technologies and skills.
Surgeons in private practice in India with pioneering mindset thus get a great opportunity to develop a leading edge practice ahead of others by early acquisition of new technologies and skills.
With opportunity comes responsibility.
Young surgeons graduating from universities have acute need for mentors who keep abreast of new developments, latest practices and advanced skills.
Senior surgeons too have limited avenues to constantly upgrade their skills unless the experts in private practice open doors to share their knowledge with their peers.
Hence the early adopters in Indian private practice have a bigger undertaking to train others compared to developed countries whose universities have resources and well oiled processes in place to lead as well as diffuse innovations.
Is it financially rewarding for Indian trainers to train their peers and juniors?
Its not. Its an honorary work where large part of expenses are borne out of pocket by trainers.
For instance, I was at Mysuru recently for five days with my team as an invited Faculty at the prestigious annual conference of Association of Surgeons of India, ASICON 2016. It was a great honor and privilege to demonstrate a surgery to an audience of 4000 people, make a presentation two days later, and be a panelist on the last day of the conference.
I did not gain financially if you calculated the travel costs of mine and my surgical team borne by me, and the opportunity cost of lost practice at Trivandrum for five days.
Next time, would I accept such invitation?
Absolutely yes!
But why?
A recent study from University of Alberta Canada, states five main factors that motivate the surgeons who want to teach:
(1) a sense of responsibility towards other surgeons
(2) an intrinsic enjoyment of teaching
(3) the need to maintain and expand one’s own knowledge base (teaching is the best way to learn)
(4) watching trainees develop into competent practitioners and playing a role in their success
(5) fostering positive lifelong professional relationships with learners.
The satisfaction from the above listed reasons far exceed the needs to feel exclusive, make huge money out of training, or nurse pride that I am superior to others by keeping my tips and tricks secret.
Apart from my regular travel to various conferences as faculty, we have been running short term and long term fellowships in Minimally Invasive Surgery at our center for many years.
So far, we have just been training the fellows who would approach us.
With the encouraging results and feedback from them, we plan to launch a formal fellowship program in the first quarter of 2017.
Our main aim is to fill confidence in talented surgeons that come to us.
We follow a three step process to do so, which has never failed in creating confident Keyhole Surgeons at the end of each fellowship.
First, we share all our tips and tricks wholeheartedly with our fellows. No withholding. You would have seen me do so in my live surgery demonstrations too. The tips could be on patient positioning, port placement, minor but vital trick in suture placing, needle holding, which hand or finger to use, where to look etc. etc. No trick is small to a learner. Besides, transparency makes a tremendous difference to the trainees’ morale and their trust in us. Its a vital foundation to build before we move forward.
Second, we provide them with first hand exposure when they are ready for it. This is a golden moment for a trainee to try newly learnt techniques slowly and safely under our guidance. Confidence starts galloping with practical exposure and now is the time to nurture it. How do we nurture the new-found confidence? Trainees need to be confident all the time; not just while operating. Their opinions must be valued. Good suggestions accepted. Training should extend to adjunct procedures- ERCP, EUS, Colonoscopy, and what not. Their good work must be showcased with opportunities to present in National and International conferences. That’s when a well rounded Laparoscopic Surgeon will emerge out of the program.
Third element of our fellowship is to develop a critical non-technical competency. Why do some surgeons outperform their peers even when technical skills are equal? Studies in healthcare show that Emotional Intelligence (EI) is the differentiation. A recent article from Dr Daniel Chiu, a gastrointestinal surgeon from the University of Alabama speaks at length about relevance of EI to surgeons and how it improves Doctor-Patient relationship amongst host of other benefits. Developing EI in our fellows is a subtle process. Many a times they may not know they are being trained. Recording all complaints, organized history taking, thorough examination, how to convey prognosis to patients, how to speak to their relatives, conveying pros and cons of available treatment options, excellent bed side manners, and auditing one’s own work for continuous excellence are some of the soft skills what we offer to our fellows to learn in this element. The idea is to start developing them as effective leaders of their future teams and empathetic care givers.
Our above three step approach over the years has been evolved into a well structured fellowship model. We call it TIDDMAS Training Model:
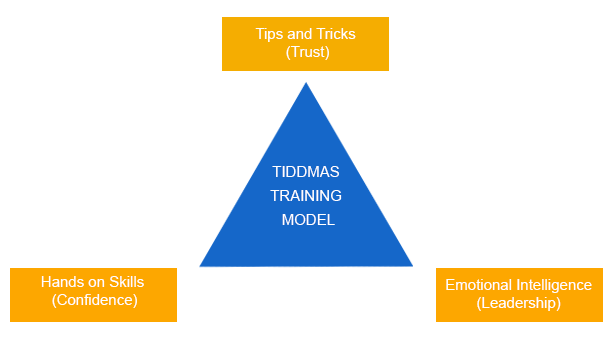
In essence, building trust, confidence and leadership in our fellows is the real substance we intend to develop through our model, by relying upon the forms of tips and tricks, hands-on exposure and emotional intelligence.
Hope we will be able to train hundreds of more fellows with the upcoming launch of our formal fellowship program so that we can make a difference to thousands of more patients through them.
That in itself is a handsome reward.
Would you agree?
Take Care
